Are B12 Injections Covered By Insurance Should you get B12 shots if you have MTHFR?
Should You Get B12 Shots If You Have MTHFR? A Cautious, Consumer-Style Guide
“Should you get B12 shots if you have MTHFR?” is getting attention for a very practical reason: MTHFR is widely mentioned in wellness spaces, and vitamin B12 is one of the supplements people connect to methylation and homocysteine support. But the search intent underneath that question is usually more personal—young women want energy, “brain fog” relief, better labs, fewer symptoms they’re tired of chasing, and a plan that feels credible without being reckless.
From a consumer-review perspective, here’s the key caution: if you have MTHFR, that doesn’t automatically mean you’ll benefit from B12 injections. B12 shots are not a personality test or a one-size-fits-all fix. They can be reasonable in specific situations—especially when B12 deficiency is confirmed, absorption is impaired, or a clinician recommends an injection-first approach. What matters most is your lab results, your diet and medication context, and how your body responds over time.
What Should You Get B12 Shots If You Have MTHFR Is and Who It Might Fit Best
To put the topic into plain terms, MTHFR refers to variations in the MTHFR gene (commonly tested as C677T and A1298C). These variations can influence folate metabolism and homocysteine pathways for some people. Separately, vitamin B12 is needed for normal cellular processes and works closely with folate metabolism.
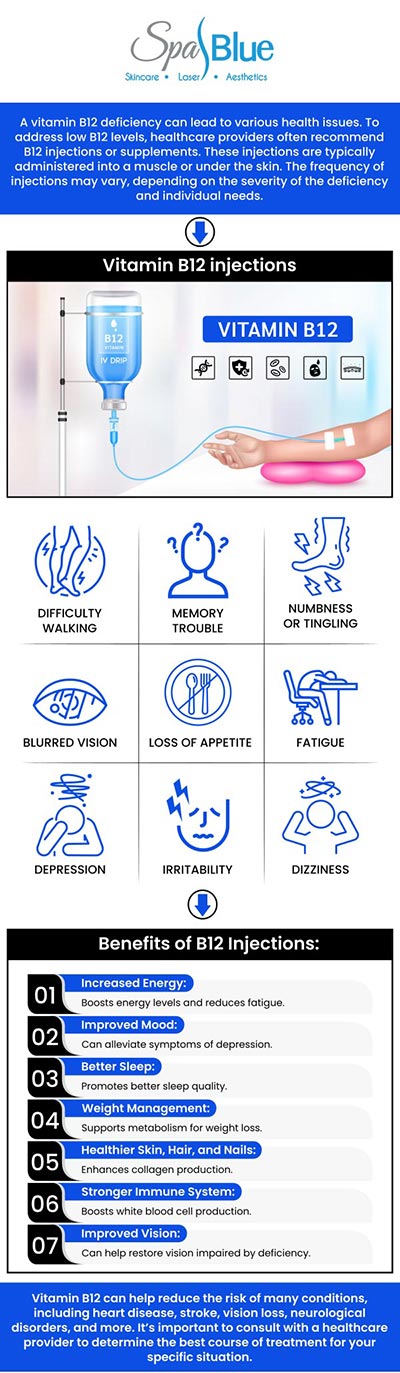
So where do B12 shots come in? B12 injections (often intramuscular or subcutaneous) are a way to deliver vitamin B12 without relying entirely on gut absorption. That’s why the injection idea tends to show up in discussions around deficiency states and absorption issues.
Who it might fit best (typical patterns I’ve seen in real-world supplement decisions):
- You have labs suggesting low B12 or borderline B12, especially if you also have symptoms that could align with deficiency.
- You have absorption risk factors (for example, certain GI conditions, long-term acid suppression, or a history that makes oral B12 less reliable).
- You want a structured approach and you’re willing to recheck labs after a defined period.
- A clinician already recommended injections based on your history, not just your genotype.
Who it might not be the best first move: If your labs are normal, diet is generally adequate, and you don’t have an absorption concern, then “B12 shots if you have MTHFR” can become an expensive detour. In that scenario, oral B12 (or targeted folate strategy) may make more sense—again, ideally guided by your lab picture.
Practical Benefits and Where It Falls Short
Let’s talk like a consumer: what you can realistically expect to feel (and what you can’t). With B12 shots, the most plausible “benefit” you might notice is improved support for pathways involved in energy metabolism and related symptoms—if your body was actually under-supplied with B12.
Personal experience case (measured improvement, not magic): A friend of mine (mid-20s, young woman, vegetarian-leaning but inconsistent) had MTHFR testing and started searching “should you get B12 shots if you have MTHFR.” Her follow-up labs showed borderline B12 and a pattern that raised her clinician’s concern about whether she was truly absorbing enough. She did a defined injection period (a typical starting course over a few weeks), then rechecked labs and tracked symptoms weekly. The positive change wasn’t “instant.” Over ~2–4 weeks she reported better stamina and fewer dizzy spells, but only after the plan was paired with more consistent diet and follow-up testing. Even then, she still described some ups and downs—suggesting B12 helped, but wasn’t the only lever.
Negative case (no benefit, side effects, and missing follow-through): Another case I saw: someone took B12 injections because she read that MTHFR means you “can’t methylate well.” Her starting B12 values weren’t clearly low, but she skipped labs and used a dosing schedule she found online. After the injections, she experienced headaches and mild nausea for a few days each time. She kept going for about a month but didn’t track symptoms systematically and didn’t recheck labs. When she finally got testing, her B12 was not low anymore, and other issues (iron status and sleep disruption) were the more obvious culprits. In her case, “B12 shots if you have MTHFR” became less like a targeted fix and more like a side-effect routine.
Where B12 shots fall short:
- If your B12 is normal, you may pay for injections without getting clear symptom change.
- Symptoms are not specific—fatigue, “brain fog,” and mood changes can come from multiple causes (iron deficiency, thyroid issues, vitamin D insufficiency, stress, sleep, medications, and more).
- Consistency and monitoring matter. A short trial without labs can’t tell you whether B12 was the missing piece.
- Dosing and form vary. Some products include additional components; mixing plans without clarity can muddle outcomes.
What Research Suggests and What It Doesn't About B12 Shots If You Have MTHFR
Here’s the evidence-grounded way to frame it: B12 is essential, and deficiency can be associated with symptoms. In populations with confirmed deficiency, supplementation (including injectable forms) can be appropriate. However, when you add MTHFR to the equation, the story becomes more nuanced.
What research generally supports:
- Correcting true vitamin B12 deficiency is important for health.
- Injection vs oral approaches can differ in practicality and absorption reliance—especially when gut absorption is uncertain.
- Lab-guided supplementation is a more reliable approach than genotype-only decisions.
What research doesn’t clearly prove for “B12 shots if you have MTHFR”:
- MTHFR variants alone automatically require injections. Most people with MTHFR do not have a universal “B12 must be injected” pathway.
- Guaranteed symptom resolution. Even in deficiency, symptom timelines vary and other causes can overlap.
- One perfect protocol. Dosing, frequency, and duration depend on what your labs show and why you’re supplementing.
Risks to take seriously (even if you’re cautious): B12 shots are generally well tolerated by many people, but side effects can occur. Also, high-dose supplementation without a clear reason can complicate the picture. If you have a history of allergies, are pregnant, or have kidney issues, you should discuss the plan with a clinician before turning injections into a routine.
Bottom line: research supports targeted correction of deficiencies, not a blanket “shots are the solution” rule for MTHFR.
Ingredients, Formats, and Quality Signals
If you’re shopping for the “B12 shots” angle, quality matters as much as the concept. Consumer experience often comes down to whether the product is consistent, clearly labeled, and sourced responsibly.
Common B12 injection formats you’ll see:
- Hydroxocobalamin injections (often discussed for longer-lasting forms)
- Cyanocobalamin injections (a common, widely used form)
- Mixes with “methyl” nutrients (sometimes includes folate variants or B-complex items—check labels carefully)
What to look for on labels and in listings (quality signals):
- Clear labeling of the B12 form (hydroxo vs cyano) and the actual amount per mL.
- Traceable manufacturer info and consistent packaging.
- Batch testing or third-party verification when available.
- Appropriate storage instructions (injections are not “shelf-stable in any condition”).
- Transparent dosing guidance that matches a medically reasonable approach.
What to be skeptical about (consumer red flags):
- Unclear dosing (“B12 high potency” with no milligrams or micrograms specified)
- Marketing that implies genotype-based cure claims
- Mixes that bundle many actives without explaining what’s in each and why
- Prices that seem too good to be true paired with vague sourcing
Practical pricing reality check: Injections can vary widely by provider and dose. A consumer-friendly way to compare isn’t just “how much per shot,” but “what you paid for the dose + supplies + follow-up plan (like rechecking labs).” I’ve seen budgets get derailed when people focus on the per-ampule price but ignore the total course cost.
Comparison of Common Options
| Format | Typical Dose/Use | Pros | Cons | Cost | Best For |
|---|---|---|---|---|---|
| B12 injection (hydroxocobalamin) | Often used in a short initial course, then maintenance based on labs | Bypasses much of gut absorption; clear delivery method | Needles, possible injection-site reactions; requires appropriate plan | Typically higher total cost than oral | Borderline/low B12 with absorption concerns or clinician-guided deficiency plans |
| B12 injection (cyanocobalamin) | Similar course/maintenance concept; varies by product strength | Common, widely available form; straightforward administration | Same injection downsides; might not align with your preferred form strategy | Often mid-range vs other medical approaches | When clinicians prefer cyanocobalamin or when it fits an evidence-based dosing schedule |
| Oral methylated B12 (tablets/capsules) | Common daily or every-other-day dosing depending on product | Convenient; no injections; generally easy to try with tracking | May be less reliable if absorption is impaired; slower to see changes | Usually lower upfront than injections | Normal-to-borderline labs, diet gaps, or anyone wanting a gentle first trial |
| Sublingual B12 | Daily dosing is common; varies widely by brand | Often easier than swallowing pills; convenient for routine | Still may rely on absorption processes; dosing transparency varies | Mid-range depending on potency | People who prefer an oral approach but want practical “routine compliance” |
| B12 in a B-complex (multi-vitamin) | Depends on formula; not always high enough for deficiency goals | More comprehensive support; can simplify your stack | May dilute B12 dose; can complicate identifying what helped | Varies from low to moderate | Maintenance when labs are okay and your goal is general coverage |
Buying Framework and Red Flags for “Should You Get B12 Shots If You Have MTHFR”
If you’re trying to decide, use a framework that protects you from spending money on the wrong problem. Think of this as a mini consumer checklist.
Buying checklist (before you commit):
- Lab context: Do you know your B12 (and ideally functional markers if your clinician uses them)?
- MTHFR clarity: Do you understand your genotype result and whether anyone is linking it to folate or homocysteine issues in your case?
- Reason for injection: Is the plan based on deficiency, absorption concerns, or clinician preference—not just a trend?
- Dose plan: Is there a defined dose and timeline, plus a plan for follow-up?
- Side-effect plan: Do you know when to stop and contact a clinician (rash, breathing issues, persistent severe headaches, or other concerning symptoms)?
- Cost transparency: Are you paying for a full course with rechecks, not just an individual shot?
- Stack compatibility: Are you combining B12 with other supplements thoughtfully (especially folate forms), rather than random add-ons?
Red flags (I’d pause here):
- “MTHFR means you need B12 shots” with no mention of labs.
- Vague dosing like “high potency” without the B12 form and amount.
- No plan to recheck labs or revisit the diagnosis after a trial.
- Claims that imply cure-level outcomes tied to genotype.
- Products that include multiple actives but don’t explain why you’d need all of them.

Common Mistakes and How to Avoid Them
- Using MTHFR as the only deciding factor: MTHFR is a piece of your puzzle, not the whole puzzle. Labs and symptoms still matter.
- Starting injections without a plan for follow-up: If you’re going to try it, set a time window (for example, 2–6 weeks depending on your clinician) and decide how you’ll evaluate response (symptoms + possibly labs).
- Ignoring side effects: Mild, transient effects can happen, but persistent reactions are a reason to stop and reassess.
- Mixing folate and B12 “because methylation”: Supplement stacks can interact in ways you might not anticipate. Make changes one step at a time.
- Expecting instant results: If you’re correcting deficiency, timelines vary—symptom improvements are not guaranteed and can lag behind lab changes.
FAQ
Is it proven that you should get B12 shots if you have MTHFR?
Not as a blanket rule. B12 shots are most supported when B12 deficiency or absorption concerns are present. MTHFR alone doesn’t automatically establish that you need injections.
How long does it take to notice changes after B12 shots for MTHFR?
If B12 deficiency is part of the issue, some people notice changes over weeks. Others see slower or minimal symptom change—especially if symptoms have other drivers.
What side effects should you watch for with B12 injections when you have MTHFR?
Potential side effects can include injection-site discomfort, headaches, nausea, or acne-like breakouts in some users. Seek medical help for severe allergic-type symptoms, worsening neurological symptoms, or persistent strong reactions.
Can you combine B12 shots with folate or other methylation supplements if you have MTHFR?
Sometimes, yes, but it depends on your labs and the specific folate form/dose. Making changes without lab context can muddy cause-and-effect.
Oral vs injection: which is better if you have MTHFR and want to try B12?
For many people, oral or sublingual B12 is a reasonable first trial when labs are borderline or normal and there’s no major absorption concern. Injections may be considered when deficiency is confirmed, absorption is unreliable, or a clinician recommends an injection-first plan.
A Practical 2-Week Experiment Framework (Without Treating the “Whole Problem”)
This is not a substitute for medical care; it’s a structure to help you decide whether B12 injections are a useful line of exploration for you. The goal is to learn something, not to guarantee results.
- Day 1: Baseline check — write down your current symptoms (0–10 scale for fatigue, brain fog, dizziness, mood), sleep quality, and anything new you’re taking. If possible, align with your clinician on what labs you’ll revisit.
- Day 2–3: Confirm your plan — verify the B12 form, dose, injection frequency, and what “success” would look like for your specific goals.
- Days 4–7: Monitor tolerability — track injection-site reactions, headaches, nausea, and any unusual changes. If you get significant side effects, pause and contact a clinician.
- Days 8–14: Track symptom trend — look for a trend rather than single-day fluctuations. If you feel worse, stop and reassess rather than pushing through.
- End of week 2: Decide your next step — if your tolerability is good and there’s a clear positive direction, ask your clinician whether to continue. If there’s no signal, consider whether B12 was the wrong lever.
Failure case examples (so you know what “not working” can look like): no symptom trend after two weeks, symptoms worsen after each injection, or your later labs confirm B12 isn’t low and another condition is more likely.
Red flag warnings to treat as “stop and reassess”: signs of allergic reaction (hives, swelling, breathing trouble), severe or persistent neurological symptoms, or any reaction that intensifies with repeat dosing.
About the Author
Harper Clinical Nutrition Editing is an editorial and review-focused nutrition content team led by a registered dietitian–style health writer who has spent years refining consumer-facing supplement guidance: dosing clarity, label interpretation, and “real-life outcome” storytelling without overclaiming. The author’s disclaimer: this article is informational and based on general knowledge and consumer-style reasoning, not on diagnosis or personalized medical advice. If you have MTHFR and symptoms you’re trying to explain, base injection decisions on your lab results, medication history, and guidance from a qualified clinician.
Discussion